Anal Fissures vs Hemorrhoids: Causes, Anatomy, Treatment, and When Surgery Is Needed
Category: Health & Medicine
Tags: Anal fissure, hemorrhoids, rectum anatomy, sphincter muscle, digestive health, constipation, surgery
Introduction
Anal pain during bowel movement is a common but often embarrassing health problem. Two conditions frequently confused with each other are anal fissures and hemorrhoids (piles). Although both affect the anal region and may cause bleeding, their causes, anatomy, and treatment are different.
An anal fissure is a small tear in the lining of the anal canal, whereas internal hemorrhoids are swollen veins inside the rectum. Understanding how these conditions occur and how the anatomy of the rectum works can help in prevention and treatment.
This article explains fissures, why they are increasingly seen in the younger generation, the anatomy of the rectum and sphincter muscles, and when surgery becomes necessary.
keep reading for more similar articles
What Is an Anal Fissure?
An anal fissure is a small crack or tear in the thin lining (mucosa) of the anal canal. It usually develops at the opening of the anus where stool exits the body.
The tear exposes sensitive nerve endings and muscles underneath. Because of this, fissures can cause:
- Severe burning pain during bowel movement
- Bright red bleeding on toilet paper
- Spasm of the anal muscles
- A feeling of tearing in the anus
The pain can last for minutes or even hours after passing stool.
fistula or anal fissures vs hemorrhoid mostly found in younger generation illustraion : fissures
Why Anal Fissures Are Increasing in Younger People
Earlier, fissures were more common in middle-aged adults, but doctors now report many cases in young adults and teenagers.
The major reasons include:
1. Chronic Constipation
Young people increasingly consume processed foods with low fiber. This leads to hard stool that can tear the anal lining.
2. Sedentary Lifestyle
Long hours of sitting—especially due to computers and mobile devices—reduce bowel movement efficiency.
3. Low Water Intake
Many young people drink insufficient water, causing dry stool.
4. Frequent Spicy or Junk Food
Highly spicy and processed foods may irritate the digestive tract.
5. Stress and Irregular Eating Habits
Stress affects gut motility and may cause constipation.
All these factors increase the risk of developing fissures.
Difference Between Anal Fissure and Internal Hemorrhoids
Although both conditions may cause bleeding, they are very different.
| Feature | Anal Fissure | Internal Hemorrhoids |
| Main problem | Tear in anal lining | Swollen veins inside rectum |
| Pain | Severe pain during stool | Usually painless |
| Bleeding | Bright red streak on stool | Drops of blood in toilet |
| Cause | Hard stool or trauma | Pressure on rectal veins |
| Location | Anal canal opening | Inside rectum |
Hemorrhoids are mainly vascular swelling, whereas fissures are tissue tears.
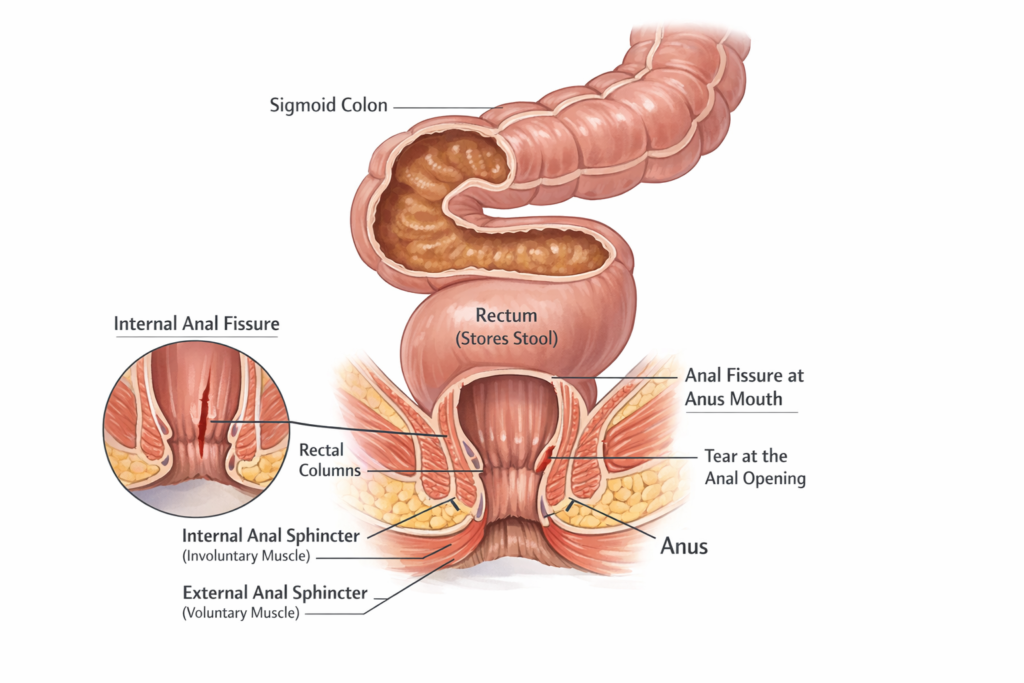
Anatomy of the Rectum and Anal Canal
To understand fissures, it is important to know the structure of the lower digestive tract.
1. Sigmoid Colon
The sigmoid colon is the S-shaped final part of the large intestine. Its main functions are:
- Storing fecal matter before elimination
- Absorbing water and electrolytes
- Moving stool into the rectum through muscular contractions
When stool stays too long in the sigmoid colon, excess water is absorbed, making stool hard and difficult to pass.
2. Rectum
The rectum is the final straight portion of the large intestine, about 12–15 cm long.
Functions include:
- Temporary storage of feces
- Signaling the brain when bowel movement is required
- Coordinating the opening of the anal canal
Inside the rectum are folds called rectal columns or columns of Morgagni. These columns contain blood vessels and connective tissue.
Internal hemorrhoids develop from the swelling of these vascular structures.
3. Anal Canal
The anal canal is the last 3–4 cm of the digestive tract. It ends at the anus.
It contains very sensitive nerves, which is why any injury such as fissures causes intense pain.
Sphincter Muscles
Two circular muscles control the opening and closing of the anus.
Internal Anal Sphincter
- Involuntary muscle
- Always partially contracted
- Maintains continence
External Anal Sphincter
- Voluntary muscle
- Controlled by the brain
- Allows conscious control over bowel movement
When a fissure forms, the internal sphincter goes into spasm. This spasm reduces blood supply to the wound, preventing healing and causing repeated pain.
Internal Fissure vs Anal Mouth Fissure
Fissures usually occur at specific locations in the anal canal.
Posterior Fissure (Most Common)
Occurs at the back of the anal opening. About 90% of fissures occur here.
Anterior Fissure
Occurs at the front side of the anus.
Internal Anal Fissure
If the tear extends deeper inside the anal canal, it is sometimes referred to as an internal fissure.
Anal Mouth Fissure
A fissure located directly at the outer anal opening is sometimes called an anal mouth fissure.
Both types cause similar symptoms but may differ slightly in location.
Why Fissures Take Longer to Heal
Unlike cuts on other parts of the body, fissures often take longer to cure.
The reasons include:
1. Constant Mechanical Stress
Every bowel movement stretches the wound again.
2. Muscle Spasm
Sphincter muscle spasm reduces blood flow needed for healing.
3. Bacterial Exposure
The anal region contains bacteria that can delay healing.
4. Chronic Constipation
If constipation continues, the fissure keeps reopening.
Because of these factors, fissures may become chronic, lasting for weeks or months.
Frequent Recurrence of Fissures
Some patients experience fissures repeatedly. This may occur due to:
- Persistent constipation
- Inadequate fiber intake
- Anal muscle tightness
- Inflammatory bowel disease
- Chronic diarrhea
Lifestyle modification plays a major role in prevention.
Treatment Options
Most fissures heal without surgery.
Conservative Treatment
Doctors usually recommend:
- High-fiber diet
- Drinking 2–3 liters of water daily
- Stool softeners
- Warm sitz baths
- Topical medications that relax the sphincter muscle
Many fissures heal within 4–6 weeks with these treatments.
When Is Surgery Recommended?
Surgery may be considered if:
- Fissure persists for more than 6–8 weeks
- Severe pain continues despite medication
- Chronic fissure with scar tissue develops
- Frequent recurrence occurs
- Muscle spasm is very strong
The most common procedure is called lateral internal sphincterotomy.
In this surgery, a small portion of the internal sphincter muscle is cut to reduce pressure and improve blood supply to the fissure.
Is Surgery 100% Successful?
Surgery for fissure has a very high success rate, usually 90–95%.
Benefits include:
- Rapid pain relief
- Faster healing
- Reduced recurrence
However, no surgery is absolutely 100% guaranteed.
Possible risks include:
- Minor infection
- Temporary leakage of gas
- Rare cases of stool incontinence
With experienced surgeons, complications are uncommon.
Prevention Tips
Fissures are largely preventable through healthy bowel habits.
Key prevention strategies include:
- Eating high fiber foods (vegetables, fruits, whole grains)
- Drinking adequate water
- Avoiding prolonged sitting on the toilet
- Exercising regularly
- Treating constipation early
These simple measures maintain smooth bowel movement and protect the anal lining.
Conclusion
Anal fissures are painful but usually manageable conditions caused by tears in the anal lining. They differ significantly from hemorrhoids, which involve swollen veins in the rectum.
Modern lifestyle factors—especially constipation, poor diet, and sedentary habits—are increasing fissure cases among young people. Understanding the anatomy of the rectum, sigmoid colon, and sphincter muscles helps explain why fissures cause severe pain and why healing may take time.
Most fissures respond well to dietary changes and medication. Surgery is recommended only in chronic cases but offers excellent success rates when required.
Maintaining healthy digestive habits remains the best way to prevent fissures and ensure comfortable bowel health.
References
- National Institute of Diabetes and Digestive and Kidney Diseases – Digestive Diseases Information
- Cleveland Clinic – Anal Fissure Medical Guide
- Mayo Clinic – Hemorrhoids and Anal Fissures Clinical Overview
- World Gastroenterology Organisation – Gastrointestinal Disease Guidelines
Good 👍
Very nice
Nice
Good 👍
Super
Very very nice
Good
Very good
Super 👍
Best of best
Accha hai Blog
Good 👍
Good good good good good 👍
Good 😊😊😊😊😊😊😊
Very nice
Acha hai
Very nice
Super
Nice
Good 👍
Nice nice nice nice nice nice nice nice nice nice nice nice nice 👍
Very very good
Good Sir